Lessons from Global Co-RIG: Building capacity in family medicine during a global pandemic
A Global Pandemic Response: A message from CFPC and the Besrour Centre

| The Global COVID-19 Pandemic Response and Impact Grant (Co-RIG) Program is driving family medicine and primary care innovations in low- and middle-income countries to reduce the pandemic’s impact on vulnerable communities, while informing family medicine planning and implementation globally. |
| Dear colleagues, In 2020, the Besrour Centre for Global Family Medicine at the College of Family Physicians of Canada™ (CFPC), in partnership with the Foundation for Advancing Family Medicine (FAFM), launched the Global Co-RIG Program to fuel family medicine innovations around the world. Two phase I projects were identified to respond to a crisis in patient care caused by the pandemic’s upheaval of health systems and community services. The selected projects focus on patients with chronic diseases in vulnerable communities in Indonesia and South Africa. Preliminary results indicate both projects are building capacity, improving patient care, and empowering communities through strong networks that draw on interdisciplinary teams, family members, and the wider community. By mobilizing and integrating resources in and out of the clinic, the projects reinforce the power of the Patient Medical Neighbourhood model, known globally as community-oriented primary care. The lessons emerging from two contexts as diverse as Indonesia and South Africa are not only remarkable in their similarity to each other, but also for their similarity to the 15 Co-RIG Phase I projects conducted in Canada. Working in different settings, all Co-RIG projects are advancing practice innovations, strengthening continuity of care, enhancing equity, and integrating health systems. They all demonstrate that family physicians and family medicine are indeed agents of change. As we enter year three of the pandemic and the world vacillates between acute and chronic phases of this global crisis, we are excited to see how these Global Co-RIG projects evolve and, equally, how Global Co-RIG Phase II—launching in 2022—will continue to advance family medicine innovations in low- and middle-income countries. We see a clear imperative to advance family medicine-led team models to combat ongoing impacts of the pandemic, including on mental health. We invite you to delve into the richness of learnings included in this report, and consider how they apply to your own context. Please join us also in thanking the FAFM and the Fondation Docteur Sadok Besrour for the funding that makes Global Co-RIG possible. Sincerely,
|


Global Co-RIG: A Snapshot of Impact
|
“Over half of the world’s population does not have access to health services best provided through primary care. When diseases go undiagnosed and unaddressed, individuals, families, and communities bear the burden. The situation is worsened during a global health crisis like the COVID-19 pandemic—with people in situations of vulnerability experiencing both worsening impact from COVID-19 and worsening access to routine health services.”
Dr. Shannon Barkley, Technical Officer for Primary Care, World Health Organization Shortly after the World Health Organization declared a global pandemic in 2020, the FAFM and the Besrour Centre for Global Family Medicine recognized the urgent need to support family medicine’s pandemic response in at-risk communities around the world. Inspired by the Canadian Co-RIG program, developed by the FAFM, with the generous support of the CMA Foundation, the Besrour Centre launched Global Co-RIG. The goal is to drive family medicine and primary care innovations that reduce the impact of COVID-19 on vulnerable communities in low- and middle-income countries and inform family medicine planning and implementation globally. Global Co-RIG Phase I granted two projects, $50,000 each, to tackle challenges of chronic disease management made more acute by the pandemic in their communities.  Aceh, Indonesia: Dr. Ichsan Ichsan, a family physician based in Aceh, Indonesia, observed the difficulty of caring for patients with chronic illnesses living in remote and often inaccessible areas. He and his team developed a program to educate and support a cadre of community health workers—mostly women—who in turn work with patients and their family members to support disease management in the community. Aceh, Indonesia: Dr. Ichsan Ichsan, a family physician based in Aceh, Indonesia, observed the difficulty of caring for patients with chronic illnesses living in remote and often inaccessible areas. He and his team developed a program to educate and support a cadre of community health workers—mostly women—who in turn work with patients and their family members to support disease management in the community. Cape Town, South Africa: Dr. Klaus von Pressentin and colleagues at the University of Cape Town and Stellenbosch University in South Africa are collaborating with Western Cape Government’s Metro Health Services to advance a local community health program that delivers medication, education, and COVID-19 testing in low-income neighbourhoods. They are studying the program’s impact on patients with Type 2 diabetes - a disease that impacts many South Africans and puts them at risk of significant complications from COVID-19. Cape Town, South Africa: Dr. Klaus von Pressentin and colleagues at the University of Cape Town and Stellenbosch University in South Africa are collaborating with Western Cape Government’s Metro Health Services to advance a local community health program that delivers medication, education, and COVID-19 testing in low-income neighbourhoods. They are studying the program’s impact on patients with Type 2 diabetes - a disease that impacts many South Africans and puts them at risk of significant complications from COVID-19.“The Global Co-RIG projects have demonstrated how the patient medical neighbourhood model can effectively support continuity of care in communities where access to health care is challenged by under-resourcing, logistical issues and restricted by the pandemic. Where established health systems are not sufficient to meet the needs of patients with chronic illnesses, community-based networks are powerful resources to build capacity and deliver care.”
Dr. Brady Bouchard, CFPC President, Northwest Area Family Medicine Department Lead and the Pandemic Site Lead for the Saskatchewan Health Authority.
Dr. Ichsan and Dr. von Pressentin’s innovations in community-based care are reducing the impact of COVID-19 by catalyzing change in their local communities, and reinforcing the central role of comprehensive family medicine and primary care in the global pandemic response. |
 Advancing practice innovation: Leveraging the power of community and trusted relationships to deliver care, the projects employ resource-efficient approaches to patient-centred care and translatable lessons to support rapid scale and spread of program innovations.
Advancing practice innovation: Leveraging the power of community and trusted relationships to deliver care, the projects employ resource-efficient approaches to patient-centred care and translatable lessons to support rapid scale and spread of program innovations.Empowering Community Care in Indonesia

“Family members and community leaders have well-established trusting relationships with patients. By teaching and empowering them to be partners in patient care, we can better support chronic disease management. It also shifts people’s relationship with health, wellness and family medicine.”
Dr. Ichsan, Project Lead, Family Physician, Prince Nayef Hospital and Public Health Centre, USK, Banda Aceh and Researcher, Universitas Syiah Kuala Access to primary care in rural areas is an ongoing challenge that was exacerbated by the COVID-19 pandemic and by the inequitable availability of vaccines. People with chronic disease face worse outcomes from both COVID-19 infection and reduced access to care. With funding from Global Co-RIG, Dr. Ichsan and his colleagues at the Universitas Syiah Kuala established the Family’s Health Cadre Empowerment Program to build bridges between family physicians and patients with chronic illnesses living in remote areas of Aceh, Indonesia. This program addresses urgent needs stemming from the pandemic as well as provides practical long-term solutions to strengthening patient access to primary care in low- and middle-income contexts. Cadre coordinators—mostly women—are trained by family physicians to provide public health support in their communities. They train and work with family members to monitor patient symptoms and act as a link between patients and their regular care providers to better manage disease. Use of the public “E-Health” system and phone call consultations improve access to care and strengthen connections between the health care team and patients living far away from the clinic. In a country where the public health system has not typically focused on patients with chronic illness, the program is improving disease management and reducing the risk and spread of COVID-19 within the community. Once fully implemented in 2023, the program will support 540 tuberculosis, hypertension, and diabetes-affected households in the province of Aceh. Dr. Ichsan’s work also resulted in the creation of a family medicine residency program at the Universitas Syiah Kuala in Aceh, which will further enhance primary care capacity in the region. 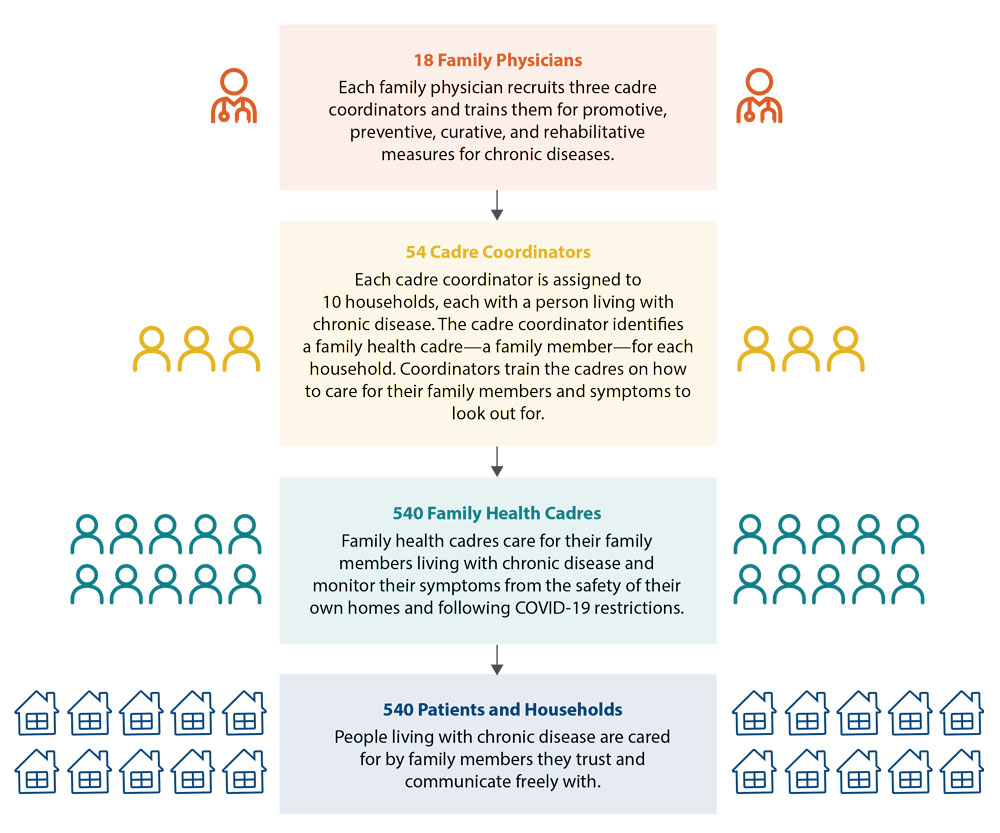 |
-
Project Impact
-
Better disease management for patients with chronic conditions that will be sustained post-pandemic
-
Stronger integration of public health and primary care
-
Enhanced relationships between family physicians and their patients
-
Strengthened communities by empowering women as leaders and caregivers
-
Strengthened community resilience to manage chronic disease in the face of future disasters
-
Increased primary care capacity through a new residency program at Universitas Syiah Kuala
-
Creation of evidence-based, scalable program
-
Strong program uptake with 40 per cent (18) of family physicians participating from the Aceh region
A trusted connection to care
Ramli, age 62, has tuberculosis. He lives in Aceh Province with his wife, Indah, and their children in a rural community that is hours away from the closest public health centre. Securing reliable transportation into town is an ongoing struggle. Afraid of COVID-19, Ramli stopped attending monthly medical appointments. Unaware of symptoms of worsening tuberculosis or the impact of inconsistent use of medication on health outcomes, Ramli’s health rapidly deteriorated.
A cadre coordinator from the public health centre contacted Indah and trained her to monitor Ramli’s disease and provided educational resources to support her care. Using her newly developed skills, Indah helped Ramli adhere to his medication regimen, preventing his tuberculosis from worsening.“This fascinating project influenced the establishment of our family medicine residency study program, which we hope to have up and running in 2022. Support from the FAFM and the Besrour Centre was instrumental in helping us initiate this program.”
M. Yani, M.Kes, PKK, SpKKLP, Head, Family Medicine Residency Program and Chief, Association of Indonesian Family Physicians, Aceh Chapter -
-
Project Tools
“As a leader in my community, I am very excited by this project. A partnership among family physicians, health cadre, and religious leaders in solving issues related to chronic disease has never been done before. Incorporating health lessons into our religious lectures will help educate our community and improve health-seeking behaviour and treatment trajectory. Bismillah!”
TGK, religious leader in Aceh District
A community approach: The community medical home model of care draws on existing relationships between physician, patient, and family member. Engaging local community leaders to serve as key information sources supports program success.

Recruitment: Flyers, booklets, and videos developed in collaboration with the Universitas Syiah Kuala of Banda Aceh help patients and cadres and support the recruitment of family physicians to the program.

Digital: Cadre coordinators use “E-health”, a telecommunication program established by the Indonesia Family Doctors’ Association, to stay in touch with their primary care team and cellphone message groups facilitate information sharing and health consultation with patients.

Knowledge mobilization: A train-the-trainer program ensures a consistent approach to cadre coordinator training and enhances cadre communication skills, professional development, and teamwork. The program can also help others implement a similar program in their region or country.
-
Project Team
- Project Lead: Dr. Ichsan, Department of Family Medicine, Faculty of Medicine, Universitas Syiah Kuala
- Amanda Yufika, Department of Family Medicine, Faculty of Medicine, Universitas Syiah Kuala
- Syahrizal, Department of Family Medicine, Faculty of Medicine, Universitas Syiah Kuala
- Zahratul Aini, Department of Family Medicine, Faculty of Medicine, Universitas Syiah Kuala
Family Medicine, Chronic Disease and COVID-19: Strengthening diabetes management in South Africa
-
Project Impact
- Reduce mortality and morbidity for patients with type 2 diabetes including improved cardiovascular and kidney health, neuropathy, and vision.
- Establish an innovative method to optimize supportive care for at-risk patients in communities lacking access to primary health care.
- Demonstrate the value of digital networking tools to connect patients with their care teams.
- Improve patient outcomes through strengthened medication access and educational supports, critical elements in vulnerable populations with multiple comorbidities.
- Reduce the impact of COVID-19 in target households through education and regular screening.
- Reinforce the importance of synergistic support services to reduce COVID-19 complications for at-risk patients.
- Facilitate diabetes self-management for stable patients.
Helping Maria manage her diabetes at home
Maria, age 80, has type 2 diabetes and is in constant pain due to diabetic neuropathy. Living in a low-income neighbourhood with inadequate public transportation, even before the pandemic, Maria struggled to get medication from the health clinic. Early on during the pandemic, a community health worker started weekly visits with Maria to monitor her diabetes, deliver medication and counselling, screen her household for COVID-19 and arrange telephone appointments with a family physician as needed.
Maria was also invited to participate in the evaluation of the program. Following guidelines provided by the healthcare team, Maria can adhere to her diabetes medication schedule and make lifestyle changes that improve her diabetes management. COVID-19 education and regular screening of her household reduce the risk of serious virus-related outcomes. She also feels empowered to be participating in research to help patients like her.“Pandemic lockdowns led to the sudden de-escalation of primary health care services in the Western Cape and routine primary care services became inaccessible to many patients almost overnight. Community health workers took on the heroic role of bringing health care to the homes of patients. They strengthened parts of community-oriented health care in areas where this was previously non-existent and became critical ‘eyes and ears’ in the community, linking patients in need to surrounding clinics.”
Dr. Haneem Salie, primary care doctor at a participating facility, MHS -
Project Tools
“The overwhelming majority of patients interviewed during the evaluation live in dire socio-economic conditions that are compounded by high rates of unemployment and compromised access to in-home sanitation. Many of these households depend on government grants, which are stretched to feed four to six people.”
Li’Tsoanelo Zwane, project research assistant
Home delivery of medication: With clinics in four low-income neighbourhoods in Cape Town, 2,500 community health workers deliver pre-packaged medication to patients to improve medication adherence and protect patients from exposure to COVID-19.

Patient education and counselling: Helping patients to understand the importance of behaviour changes is critical to empowering people with type 2 diabetes and other chronic diseases to better manage their medication and make necessary lifestyle changes.

Household COVID-19 screening and testing: Ongoing screening and testing of households by community health workers helps with early diagnosis of COVID-19 infection, reduces the risk of transmission, and helps to protect patients with diabetes, who are at risk for worse COVID-19 outcomes.

Digital health: Telephone consultations between family physicians and patients, coupled with digital applications such as WhatsApp, help patients receive care using the technology available to them.

Evaluation: Flyers, targeted outreach by community leaders, and a small stipend supported evaluation, recruitment, and participation by patients with information collected over the telephone.
-
Project Team
- Project Lead: Associate Professor Dr. Klaus von Pressentin, Division of Family Medicine, School of Public Health and Family Medicine, Faculty of Health Sciences, University of Cape Town
- Professor Bob Mash, Division of Family Medicine, Faculty of Medicine and Health Sciences, Stellenbosch University
- Dr. Neal David, Division of Family Medicine, School of Public Health and Family Medicine, Faculty of Health Sciences, University of Cape Town
- Adjunct Associate Professor Graham Bresick, Division of Family Medicine, School of Public Health and Family Medicine, Faculty of Health Sciences, University of Cape Town
- Natasha Moodaley, Research Project Manager, Faculty of Health Sciences, University of Cape Town
- Deon September, Research Assistant, Division of Family Medicine, School of Public Health and Family Medicine, Faculty of Health Sciences, University of Cape Town
- Li’Tsoanelo Zwane, Research Assistant, Division of Family Medicine, School of Public Health and Family Medicine, Faculty of Health Sciences, University of Cape Town
- Naledi Makhafula, Research Assistant, Division of Family Medicine, School of Public Health and Family Medicine, Faculty of Health Sciences, University of Cape Town
- Dr. Omotayo Alaofin, postdoctoral fellow, Division of Family Medicine, School of Public Health and Family Medicine, Faculty of Health Sciences, University of Cape Town
- Dr. Haneem Salie, primary care doctor at a participating facility, MHS; lecturer, Division of Family Medicine, School of Public Health and Family Medicine, Faculty of Health Sciences, University of Cape Town
- Dr. Beverley Schweitzer, family physician at a participating facility, MHS; senior lecturer, Division of Family Medicine, School of Public Health and Family Medicine, Faculty of Health Sciences, University of Cape Town
- Dr. Leigh Wagner, family physician at a participating facility, MHS; senior lecturer, Division of Family Medicine and Primary Care, Faculty of Medicine and Health Sciences, Stellenbosch University
- Dr. James Porter, family physician at a participating facility, MHS; senior lecturer, Division of Family Medicine and Primary Care, Faculty of Medicine and Health Sciences, Stellenbosch University
Dr. Klaus von Pressentin, Project Lead, Associate Professor, University of Cape Town
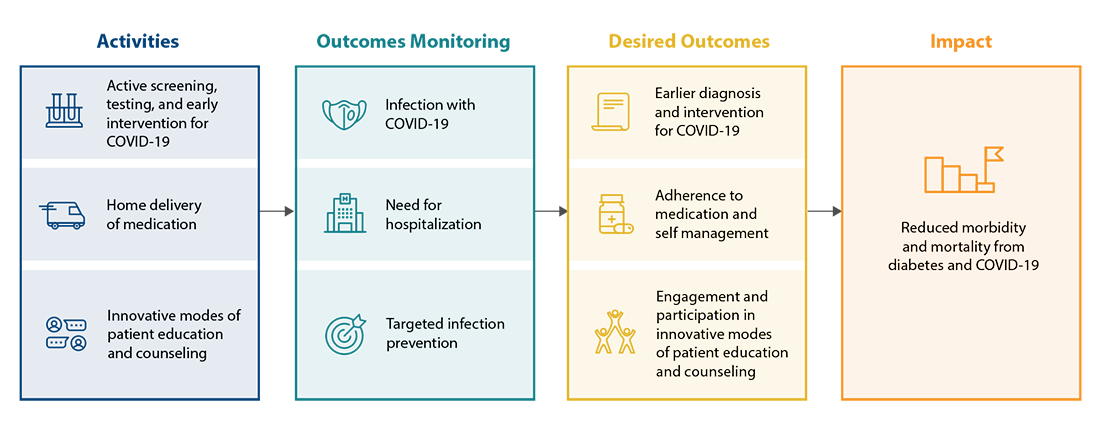
Early in the COVID-19 pandemic, the Western Cape Government’s Metro Health Services (MHS) launched an innovative community-based health program to reduce the impact of chronic disease and COVID-19 in low-income Cape Town neighbourhoods.
The program uses a network of 2,500 community health workers to support households impacted by chronic diseases in four at-risk communities. Community health workers deliver pre-packaged medication, provide disease and pandemic-related education, and screen households for COVID-19. Health workers also connect patients with counselling and health care supports as required.
Recognizing the program’s potential to improve patient health, Dr. Klaus von Pressentin and colleagues at the University of Cape Town and Stellenbosch University collaborated with the MHS to study the program’s impact. They focused on patients with type 2 diabetes as this is a large population in South Africa and it’s at particular risk for poor outcomes from COVID-19 infection.
Input was collected from 269 patients with type 2 diabetes to help assess the outcomes of the overall program. Patients were asked about the method of medication delivery; the ability to self-manage their diabetes by adhering to medication and lifestyle modifications; how COVID-19 screening, and education minimized the risk of COVID-19; and the impact of using technology for consultations.
Data and other inputs are being analyzed to assess the program’s impact on supporting patients to self-manage their disease, and the potential for the program to optimize primary care services to improve health outcomes in low-income communities.
Almost overnight, the innovative project brought primary care to areas that had been underserved. Patients are being linked to a team of health care workers and health clinics and empowered to manage their disease. With MHS as a partner, the evaluation increases the potential for the project to be quickly scaled up throughout Cape Town and replicated elsewhere in South Africa or beyond. As the world looks past the pandemic, lessons learned can inform emergency planning for future public health crises.
Global Co-RIG Phase II

Marie-Dominique Beaulieu, CQ, MD, CMFC, MSc, FCMF, Co-RIG Steering Committee Chair, Professeure émérite, Département de médecine de famille et de médecine d’urgence, Faculté de médecine, Université de Montréal
As we look ahead, the Besrour Centre and its partners are committed to working with the global family medicine community to continue to drive change through innovations that prepare family physicians and interprofessional teams to cope with emergent challenges related to the pandemic and its longer-term impact.
In 2022, the Besrour Centre is pleased to be launching Global Co-RIG Phase II with focus on key aspects of the chronic phase of the pandemic, in low- and middle-income countries:
- Addressing barriers in under-served communities: In many areas of the world, low vaccination rates and limited resources remain active barriers on the road to local and global recovery from the COVID-19 pandemic. Initiatives are needed to address these barriers, improve health equity, and build capacity.
- Supporting mental health: New variants and additional restrictions exacerbate the impact of the pandemic beyond physical health. Instability due to financial insecurity, unemployment, lack of social connections, and difficulty in accessing health services take a toll on mental health. Addressing mental health needs and ensuring timely delivery of these services is of great urgency and a global priority.
- Supporting interdisciplinary primary care teams: As the first point of access to health services, family physicians and primary care teams are uniquely positioned and play an essential role in addressing the health needs of the population. Projects that build an effective network of care are critical.
Global Phase II projects are expected to launch in 2022. Check the Besrour Centre for more information.
Dr. Janet Hatcher Roberts, Co-Director, WHO Collaborating Centre for Knowledge Translation, Technology Assessment for Health Equity, Bruyere Research Institute, University of Ottawa; Adjunct Professor, School of Public Health and Epidemiology, University of Ottawa; Adjunct Professor, Department of Community Medicine and Epidemiology, Centre for Global Health, Dalhousie University.